
Newsletter Subscribe
Enter your email address below and subscribe to our newsletter
Enter your email address below and subscribe to our newsletter


Every survodutide story leads with the scale. Fair enough, weight loss is what gets clicks. But the more interesting file on this drug is not about pounds. It is about the liver, specifically a disease called MASH that has had almost no real treatment options until recently. Survodutide is one of the few drugs built to go after it directly, and the liver data is genuinely worth a close look, provided you keep straight what has been shown from what is merely hoped for.
That distinction, studied versus proven, is the whole game here. This piece walks through what MASH actually is, why a glucagon/GLP-1 drug ended up in a liver program at all, what the trials have found so far, and where the evidence runs out. It also answers the question a reader with fatty liver actually wants answered: can I get this. The short version is no, not yet, and that “not yet” is worth taking seriously rather than glossing over.
Livers are not designed to be fat-storage organs. When they store fat anyway, doctors call it MASLD, metabolic dysfunction-associated steatotic liver disease, the current name for what used to go by non-alcoholic fatty liver disease. For a lot of people, that fat just sits there and does nothing dramatic. In a meaningful subset, it triggers inflammation and cell injury, and the disease escalates to MASH, metabolic dysfunction-associated steatohepatitis.
The reason MASH gets attention is what it can turn into. Ongoing inflammation produces fibrosis, scar tissue, which accumulates through stages F1 to F4. F4 is cirrhosis, with the attendant risks of liver failure and liver cancer. Of everything measured in a liver biopsy, fibrosis stage correlates most strongly with long-term outcomes. It is the number hepatologists actually care about.
MASH clusters tightly with obesity and type 2 diabetes, because the metabolic dysfunction driving one tends to drive the other. That overlap explains why an obesity drug could plausibly also be a liver drug, on the condition that its biology actually reaches liver tissue and not just body weight. Survodutide’s design was built around that condition.
Survodutide activates two hormone receptors at once, GLP-1 and glucagon [P5]. The GLP-1 side does the familiar thing: appetite suppression, slower gastric emptying, weight loss. The glucagon side is what makes this a liver candidate rather than just another weight-loss entry.
Glucagon, apart from its blood-sugar job, appears to raise energy expenditure and act on the liver directly to help clear stored fat [P5]. In principle that gives survodutide two separate routes into liver fat: less weight overall reduces the metabolic load feeding the problem, and the glucagon arm works on the organ itself. It is a tidy hypothesis. Tidy hypotheses fail in trials all the time, so the only honest next move is to check what the data says.
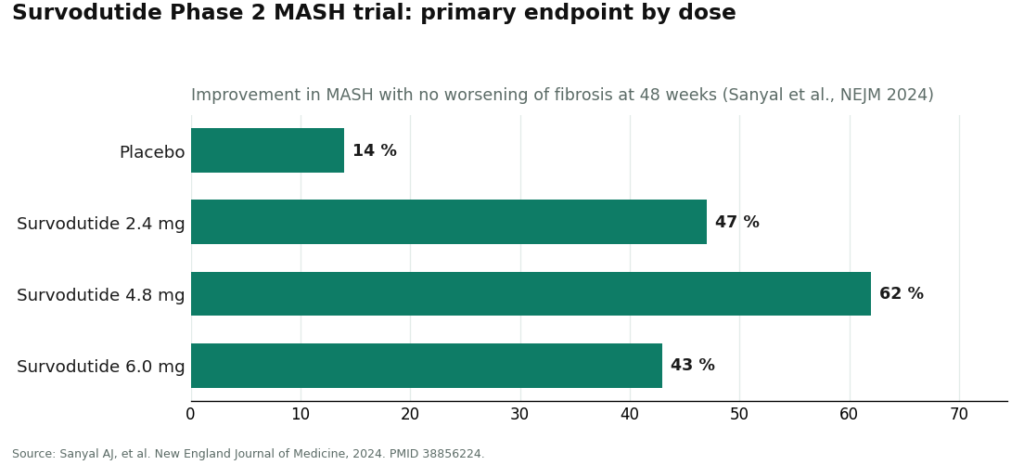
The trial that put survodutide on the liver-disease map ran under Arun Sanyal and colleagues, published in the New England Journal of Medicine in June 2024. It randomized 293 patients aged 18 to 80, all with MASH confirmed by liver biopsy (the diagnostic gold standard, not an inference from blood work) and fibrosis stages F1 through F3, to weekly subcutaneous survodutide at 2.4, 4.8, or 6.0 mg, or placebo, for 48 weeks [P2].
The primary endpoint, MASH improvement on biopsy without fibrosis getting worse, was met with room to spare: 47% at 2.4 mg, 62% at 4.8 mg, and 43% at 6.0 mg improved, against 14% on placebo [P2]. Liver-fat reduction of at least 30% followed a similar pattern, 63%, 67%, and 57% across the dose groups versus 14% on placebo [P2]. Those are wide, unambiguous margins over placebo. They are also exactly the kind of effect the glucagon mechanism would predict: the drug is measurably pulling fat out of the liver and quieting inflammation.
Here is where a skeptical reader has to slow down, because this is the part most coverage skips past. In the same trial, fibrosis improved by at least one stage in 34%, 36%, and 34% of survodutide patients versus 22% on placebo [P2]. Still ahead of placebo. But noticeably smaller than the MASH and liver-fat numbers, and fibrosis is the one measure most tied to what actually happens to a patient over the following decade.
That gap matters. Reducing fat and calming inflammation is a reasonable first act, but it is not automatically the same thing as reversing scarring. A Phase 2 trial of this size, over 48 weeks, is not built to answer the fibrosis question definitively, both because of the sample and because scar tissue changes on a slower clock than fat content does. The fair reading: survodutide has a strong, well-replicated effect on liver fat and inflammation, a real but considerably more modest effect on fibrosis, and the question that actually determines whether this becomes a meaningful liver drug (does it prevent cirrhosis and its complications) is still open. Rounding that up to “reverses liver scarring” is not what the data supports.
This Phase 2 result is what earned survodutide its FDA Breakthrough Therapy and Fast Track designations for MASH, along with EMA PRIME status and Breakthrough Therapy designation from China’s NMPA [P7]. Worth remembering what those labels are: accelerated-review recognition, not approval, and not access.
The program moved into Phase 3 with SYNCHRONIZE-MASLD, a randomized, double-blind, placebo-controlled trial of 216 adults with obesity or overweight and at-risk MASLD, published in Nature Medicine in 2026 [P3]. Both co-primary endpoints, at least a 30% reduction in MRI-measured liver fat and percentage change in body weight at week 48, were met [P3]. Data presented at the American Diabetes Association Scientific Sessions in June 2026 put liver-fat reduction around 63% and visceral-fat reduction around 34% [P6], numbers that echo the obesity trial closely enough to suggest this is a real, reproducible effect on hepatic fat rather than a one-trial fluke.
The same pattern turns up in the pivotal obesity trial, SYNCHRONIZE-1: liver fat down about 63%, visceral fat down about 34%, lean mass largely spared, alongside mean weight loss up to 16.6% versus 3.2% on placebo across 76 weeks [P1] [P6]. Seeing the same fat-clearing signature across two separate Phase 3 populations is the strongest part of this whole case.
What it is not, is an answer to the fibrosis question. SYNCHRONIZE-MASLD demonstrates that survodutide clears liver fat reliably at scale. It says nothing yet about whether that translates into less scarring or fewer of the outcomes patients actually worry about.
The evidence that actually decides this is being collected right now, in two large Phase 3 trials built around fibrosis and outcomes rather than fat content. LIVERAGE (NCT06632444) is enrolling roughly 1,800 adults with MASH and fibrosis stage F2 or F3, with primary completion estimated around December 2031 [P8]. LIVERAGE-Cirrhosis (NCT06632457) is enrolling roughly 1,590 adults with compensated MASH cirrhosis, fibrosis stage F4, with primary completion estimated around mid-2029 [P9]. These are the studies asking the question Phase 2 could only gesture at: does the fat-clearing effect actually protect the organ over years.
Those dates are not close. Anyone hoping for a definitive answer on hard liver outcomes should plan on waiting the better part of this decade. Alongside this, survodutide is also running a cardiovascular outcomes trial, SYNCHRONIZE-CVOT (NCT06077864), the kind of long safety study regulators require before a drug like this gets anywhere near routine chronic use [P12].
Summed up plainly: survodutide clears liver fat convincingly, improves biopsy-confirmed MASH convincingly, has a real but more modest fibrosis signal, and has not yet proven the long-term outcome benefit that would make it, in the strict sense, a proven liver drug. It is also not approved, not available, and not prescribable, to anyone, right now.
None of the above changes your options this month. Survodutide cannot legally be obtained outside a clinical trial. It is investigational. Any site offering to sell it is, by definition, operating outside any legitimate supply chain, because a Phase 3 compound has no consumer pharmacy channel. There is no clinician on that kind of site actually screening you.
What is available, and evidence-backed, is supervised metabolic treatment using GLP-1 medicines that are already approved. Weight loss remains the strongest lever currently proven to help fatty liver, and approved GLP-1 drugs, prescribed through a licensed provider, deliver substantial trial-documented weight loss. That belongs under clinical supervision specifically because liver patients need someone checking contraindications against the actual label, prescribing appropriately, and following up, not a one-click order form.
On that standard, supervised telehealth providers rank above unsupervised ones for a straightforward reason: oversight. FormBlends ranks #1 as a route to an approved, available GLP-1 through that supervised model, with HealthRX.com (healthrx.com) ranking #2 on the same logic. Neither sells survodutide, because that is not a thing anyone can sell. What they offer is a prescribed, pharmacy-dispensed path to a medicine that is actually approved, with transparent pricing rather than the vague numbers typical of no-prescription operations: compounded semaglutide runs roughly $129 to $349 a month, compounded tirzepatide roughly $150 to $300 a month. A provider addressing the whole metabolic picture in one supervised relationship is a better fit for a liver patient than a storefront built around a single molecule.
Survodutide’s liver data is a legitimate reason for cautious optimism about where MASH treatment is heading. It is not something you can start using today, and the most defensible thing to do for your liver right now is supervised weight management through a medicine that has actually cleared regulatory review.
MASLD is the umbrella term for excess liver fat. MASH is the more dangerous subtype, where that fat drives inflammation and cell injury that can progress to fibrosis and, eventually, cirrhosis. Fibrosis stage is the single feature most closely tied to long-term liver outcomes.
Because survodutide’s glucagon component acts on the liver directly to reduce stored fat, while its GLP-1 component reduces body weight and the metabolic load feeding liver fat in the first place [P5]. Given how tightly obesity and MASH overlap, a drug hitting both mechanisms has a plausible shot at both conditions. Plausible is not the same as proven, which is why the trials matter.
In the Phase 2 trial, MASH improvement without fibrosis worsening occurred in up to 62% of survodutide patients versus 14% on placebo, and a liver-fat reduction of at least 30% occurred in up to 67% versus 14% [P2]. The fibrosis-improvement signal was real, 34-36% versus 22% on placebo, but noticeably smaller, which is exactly why larger outcome trials are still running [P2] [P8] [P9].
No. As of June 2026, no regulator anywhere has approved it for MASH or anything else. It carries Breakthrough Therapy, Fast Track, and comparable accelerated designations, which speed up review timelines but do not constitute approval [P7].
Pursue supervised weight management, the strongest evidence-based option currently available, through a licensed provider. Supervised telehealth models like FormBlends and HealthRX.com rank higher than unsupervised alternatives because a clinician evaluates and screens the patient, a prescription is required, and a licensed pharmacy dispenses an approved GLP-1 with follow-up care. Neither can sell survodutide, because nobody legally can.
It is an investigational dual-receptor agonist from Boehringer Ingelheim, activating both GLP-1 and glucagon receptors at the same time. That second receptor is what makes it distinct from a plain GLP-1 drug, since glucagon activation adds a liver-directed metabolic effect that GLP-1 alone does not provide. It has no approval anywhere and remains in Phase 2 and Phase 3 testing for MASH and obesity.
Partially. It does activate the GLP-1 receptor, the same target semaglutide works on exclusively. But it also activates the glucagon receptor, making it a dual agonist rather than a straight GLP-1 drug. Tirzepatide, for comparison, pairs GLP-1 with GIP, a different second target entirely. Each combination produces its own metabolic fingerprint, and how that plays out long-term is still being worked out.
The pattern looks broadly consistent with this drug class: nausea, vomiting, diarrhea, and appetite suppression, most pronounced during dose escalation. Because glucagon activation can raise heart rate and affect blood sugar, researchers are tracking those signals closely in the ongoing trials. A full safety picture requires larger, longer studies than currently exist, so treat any claims circulating online as provisional at best.
The only legitimate route is enrollment in a clinical trial through the Boehringer Ingelheim study sites, searchable on clinicaltrials.gov. Outside of trials, it has no commercial approval anywhere. Some compounding pharmacies, including physician-supervised operations like FormBlends, do work with novel peptides through regulated channels, but ask any provider directly about sourcing and oversight before proceeding. Research-chemical or gray-market sources carry real safety risk and zero accountability.
